Revisiting the global state of hyperkalaemia survey
Hyperkalaemia (HK), or elevated levels of potassium in the blood1, is a common condition among cardiorenal patients.2 Left untreated, HK can result in significant and potentially life-threatening cardiovascular (CV) complications, including serious arrhythmias and cardiac arrest in severe cases. 1,3-4
In 2021, we set out to better understand the global state of HK management for people living with chronic kidney disease (CKD) and heart failure (HF). These efforts led to the global state of hyperkalaemia survey, which fielded to 1,000 patients with CKD and HK, and 500 healthcare providers (HCPs) across five countries.5
The survey results showed that about two-thirds of CKD (n=654) and HF (n=233) patients do not know that HK is a potential complication of their condition(s) and have poor recognition of common symptoms of the disease.5 This lack of awareness among patients could lead to potentially devastating impacts for some of those living with CKD or HF.
This global survey along with more recent studies show that there is still a serious need to improve hyperkalaemia care options for cardiorenal patients, especially those who are being treated with RAASi therapy.7-8
High prevalence and significant burden of hyperkalaemia among cardiorenal patients
Patients with CKD and HF often experience HK.2,6 Recent studies emphasise the unmet need in managing HK in this population because the condition is associated with increased morbidity and mortality.7
A common approach to HK treatment involves having patients adhere to a low-potassium diet. Dietary modifications alone, however, are often an insufficient way to manage HK in CKD patients. A real-world evidence study revealed that over half of patients (n=2,048) with HK and stages 3-4 CKD experienced recurrent HK within six months due to the lack of successful interventions.*,9
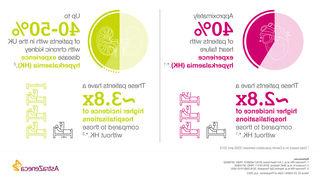
Renin–angiotensin–aldosterone system inhibitors (RAASi) therapy can be used to reduce mortality risk in HF patients and slow CKD progression while lowering cardiovascular (CV) events in CKD patients.7 RAASi therapy in patients with CKD is also linked with an increased risk of hyperkalemia.8 A HK diagnosis, however, often leads to the down-titration of RAASi therapy. Guidelines recommend the use of the highest tolerated RAASi dose, but most cardiorenal patients do not re-initiate RAASi after a HK event. Recent data shows that just 10-15% of US patients (n=25,963) and 6-8% of Japanese patients (8,722) restarted treatment within six months of an event. It is crucial to find proactive, holistic solutions for managing HK, which is why we’re diligently working to help ensure RAASi therapy can be maintained.10
Optimising care to unlock a better future for patients with hyperkalemia
During the 2023 European Renal Association congress, Ruud Dobber, Executive Vice-President, BioPharmaceuticals Business Unit, AstraZeneca, addressed the need for improved care options for patients with HK. He noted “Failing to achieve guideline-directed RAASi therapy can have serious consequences for cardiorenal patients, yet recent studies highlight how rarely these patients resume treatment following hyperkalaemia-related discontinuation, and the urgent need for practice change in hyperkalaemia management to enable this. We’re committed to supporting the management of hyperkalaemia and working with the healthcare community more broadly to help deliver better cardiorenal care for patients.”
Unlocking a better future for people with HK involves working with healthcare professionals, patient advocacy groups, governments and policymakers. This collaboration can improve access to healthcare and transform the detection, diagnosis, and treatment of HK and other CV and metabolic diseases.
At AstraZeneca, we’re working to transform outcomes for the millions of people living with the complexities of CV, renal, and metabolic (CVRM) diseases, and highlight their interconnection, including hyperkalaemia. Early detection and care are critical to improve patient outcomes and reduce the burden of CVRM diseases and their related risks and complications for patients, healthcare systems, societies, and our planet.
Disclaimer: *Data from patient populations in the United States
You may also like

References:
1. National Kidney Foundation. What is Hyperkalemia? [cited 2023 June 26]. Available from: URL: http://www.kidney.org/atoz/content/what-hyperkalemia
2. Thomsen RW et al. Nephrol Dial Transplant. 2018;33(9):1610-1620;
3. Vallentin MF, Povlsen AL, Granfeldt A, Terkelsen CJ, Andersen LW. Effect of calcium in patients with pulseless electrical activity and electrocardiographic characteristics potentially associated with hyperkalemia and ischemia-sub-study of the Calcium for Out-of-hospital Cardiac Arrest (COCA) trial. Resuscitation. 2022;181:150-157.
4. Rossignol P, Legrand M, Kosiborod M, et al. Emergency management of severe hyperkalaemia: guideline for best practice and opportunities for the future. Pharmacol Res. 2016;113(pt A):585-591. doi:10.1016/j.phrs.2016.09.039
5. Global State of Hyperkalaemia Survey Key Findings, REF-129958, AstraZeneca Pharmaceuticals LP. Veeva ID: Z4-38799. Date of preparation: October 2021
6. Furuland H, et al. BMC Nephrol 2018;19:211. PMID: 30134846
7. Kanda E, Rastogi A, Murohara T, et al. Clinical impact of suboptimal RAASi therapy following an episode of hyperkalemia. BMC Nephrol. 2023;24(1):18. doi:10.1186/s12882-022-03054-5
8. Santoro A, et al. Association between hyperkalemia, RAASi non-adherence and outcomes in chronic kidney disease. J Nephrol. 2022;35(2):463-472. doi:10.1007/s40620-021-01070-6
9. Data on file, REF-178557, AZPLP
10. Kanda E et al. Suboptimal Extent of RAASi Re-Initiation After Discontinuation Following Hyperkalemia: an Observational Study of Cardiorenal Patients in US and Japan. Presented at: ERA 2023 Congress; 2023 June 15-18; Milan, Italy.
Veeva ID: Z4-55463
Date of preparation: July 2023